Double your impact! Throughout May, your gift will be MATCHED up to $50,000, thanks to the generosity of the Robert Lloyd Corkin Charitable Foundation and our corporate partner Stryker. Make a gift today to propel research and treatments forward.
Cookie Policy
This website uses cookies that help the website function and that help us understand how you interact with it. Please read our privacy policy for more information.
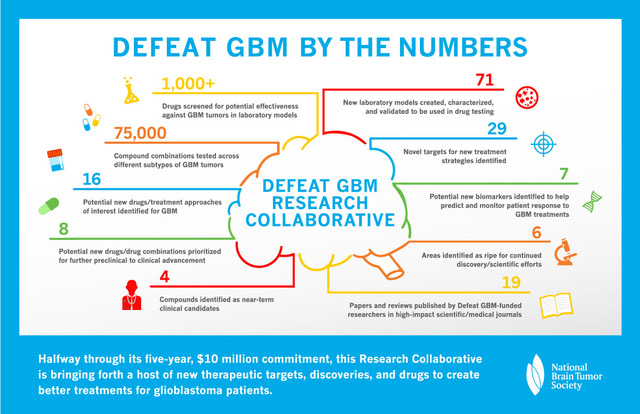
Just a few weeks ago, we provided a comprehensive update on the discoveries and advances being made by Defeat GBM (and an infographic), our flagship research program. Defeat GBM utilizes a unique infrastructure consisting of four teams, or “Cores,” of researchers that work in concert on complementary research projects, which, combined, seek to discover and then develop new potential treatments that can help glioblastoma patients. Now, we want to break down the progress more completely by looking, in context, at the accomplishments of each Core.
Like the overarching theme of the previous two Core’s work, the research in the Predictive Biomarkers Core centers on understanding why previous attempts to treat glioblastoma with targeted therapies have been unsuccessful, and to use this information to guide more successful medical approaches.
Dr. Paul Mischel at the 2016 NBTS Scientific Summit
A biomarker (short for “biological marker”), is a biological molecule found in the body that is a sign of a normal or abnormal process, or of a condition or disease. A biomarker may be used to see how well the body responds to a treatment for a disease or condition. For example, a high body temperature is a biomarker for an infection in the body, and high blood sugar is a biomarker for diabetes – conversely, lower blood sugar numbers in a diabetic can be a biomarker of response to diabetes medicines (meaning they are working).
In the context of glioblastoma, researchers want to find molecular biomarkers in the tumor cells (and/or possibly in body fluids such as blood and cerebrospinal fluid), that would predict that a patient is more likely to respond to a certain treatment, meaning any patients that have that specific marker are more likely to benefit from the medicine than others who don’t have the marker (a predictive biomarker); or a molecule whose presence indicates a patient is likely to be resistant ,or to develop resistance, to the effects of a given medicine (a biomarker of resistance). Additionally, in early phase clinical trials, researchers want to determine whether a potential medicine is working on its therapeutic target in the tumor, which can also help in optimizing the right doses of medicines for patients (a “pharmacodynamic” marker).
Unfortunately, though we know a lot about the underlying, basic biology of glioblastoma cells, we don’t have much in the way of biomarkers that can help predictively tell us ahead of time if a treatment is likely to work or not, and in which patients.
The knowledge base is incredibly deep in many ways. The map of the genes that make proteins, and their alterations, in this cancer has largely been identified. So one would expect or anticipate that this would actually make a difference in the lives of patients. But for a variety of reasons…that information has yet to really benefit patients.
Thus, the overall aim of Drs. Mischel, Cloughesy, and their collaborators’ research – though the science is very sophisticated – is actually quite simple: address the knowledge gaps in why treatment that should have worked, didn’t and learn from the past. This will inform more effective treatments for glioblastoma patients in the future.
Specifically, their team aims to:
Develop a better understanding of the mechanisms inside glioblastoma cells that can determine whether a cell is sensitive or resistance to treatments.
Use these mechanisms as biomarkers to guide more effective treatments, including using combinations of medicines to overcome resistance.
Integrate these predictive biomarkers into state-of-the-art clinical trials to improve the outcome for glioblastoma patients.
In response to the mechanistic studies from their labs, the project has progressed in a number of new, exciting and clinically actionable directions: 1) targeting tumor co-dependencies to develop more effective treatments for glioblastoma patients; and 2) determining the role of cancer-causing genes located on “extrachromosomal DNA” in glioblastoma development and growth.
Targeting Tumor Co-Dependencies
A lot of the Biomarkers team’s work is based on research findings that discovered the role EGFR mutations and alterations play in driving glioblastoma tumors, at least in part, by changing the way tumor cells take up and utilize nutrients to foster their rapid growth. As such, glioblastoma cells may become dependent on specific enzymes, proteins, and other molecules that are not themselves cancer-causing or cancer-promoting but fuel tumor growth nonetheless. This process, known as “non-oncogene addiction” or “non-oncogene co-dependency,” is a potentially very important area for study and exploitation because it could open up the potential number, and types, of drugs that could be used to treat glioblastoma beyond traditional cancer drugs.
Dr. Timothy Cloughesy at the 2016 NBTS Scientific Summit
Tumor co-dependencies can be shaped both by how a cancer causing gene – like a mutated EGFR gene – can prompt changes to a tumor’s metabolism, and by the local cellular environment around tumor cells (refer to the discussion of tumor “microenvironment in the first blog in this series). Specifically, the team believes from their studies that the unique metabolic environment of the brain itself may present actionable vulnerabilities that can be exploited with medicines to treat glioblastoma. Importantly, the Biomarker team has identified two actionable glioblastoma co-dependencies, each of which has potential to be tested in the clinic.
A cholesterol co-dependency
Twenty-percent of the body’s cholesterol is found in the brain. But cholesterol cannot get into the brain from elsewhere in the body (because of the blood-brain-barrier), meaning the brain must generate its own cholesterol for consumption. The Biomarkers team found that glioblastoma cells rely on an increased uptake of cholesterol that brain generates, creating a dependency. Glioblastoma cells are able to “re-program” the regular process for cholesterol uptake that would normally limit the amount each cell takes in. This adaptation gives glioblastoma tumors the fuel they need to keep growing out-of-control, but, importantly, it also leaves them vulnerable to drugs that could “switch back on” the normal mechanism that controls cholesterol uptake. The team is now pursuing a potential medicine that could do just that for an early-phase clinical trial.
EGFR, which we’ve talked much about in this series, is a growth factor receptor and is mutated or altered in 50-60% of all glioblastoma tumors. The most common EGFR mutation is known as “EGFRvIII.”
The Biomarkers team hypothesized that EGFRvIII causes cancer through an integrated series of events, including altering the cell’s internal signaling network, its uptake and use of nutrients, key elements of its gene-reading machinery known as transcription factors, and its epigenetic landscape – the distribution of chemical tags that determine which parts of its genome are available for reading.
To find the nodes connecting these processes and see if they could be targeted by medicines, the Biomarkers team mapped how EGFRvIII mutations change the processes in which the genetic code, stored in DNA, is transcribed into the instructions that regulate cell functions – as well as, importantly, how these multiple processes converge and might be exploited with new treatments.
Dr. Mischel
Specifically, the researchers found through scientific analysis that an EGFRvIII mutation causes changes to the landscape of “enhancers” in such a way that increases their function in glioblastoma cells. Enhancers are regions of DNA that when bound by activator proteins boost the activity of other genes . The altered group of enhancers “turned on” by the EGFRvIII mutation serve as sites where a number of different “transcription factors” – proteins that regulate the process whereby a genetic sequence of DNA is read and interpreted for its instructions – can bind, or attach themselves, to. Two transcription factors in particular that were found to be attracted to these altered enhancer sites are known as “SOX9” and “FOXG1.”
So, while an EGFRvIII mutation changes which enhancers are altered in a GBM cell, the mutation, at the same time, noticeably increases the activity of SOX9 and FOXG1 in the cell. Together, these processes serve to change the mix of genes expressed by GBM cells versus healthy cells. These results identify the role of transcriptional/epigenetic remodeling in EGFR-dependent tumor growth and suggest a mechanistic basis for epigenetic therapy.
More importantly, the team determined that it might be possible to use a drug to silence the effects of SOX9 and FOXG1.
To do so they would have to identify which genes, specifically, have their expression regulated by SOX9 and FOXG1. One of the genes they found was BRD4. The BRD4 gene, when expressed, creates a protein by the same name and controls the expression and activity of another transcription factor called cMyc, which Dr. Mischel has shown previously to play a central role in reprogramming metabolism and the growth of glioblastoma cells.
If you recall from the first blog in this series, a group of proteins known as bromodomains – and a family of bromodomain proteins know at the BET family – are thought to cause glioblastoma treatment resistance. The BRD4 protein is part of the BET family. Thus, the team wants to gain a deeper understating of, and evaluate, potential drugs that target BET proteins and if they could work for glioblastoma patients. They point out that there is an added advantage of having a predetermined biomarker – the presence of EGFRvIII – to determine which patients are most likely to benefit from the treatment.
Further, the identification of two master transcription factors, SOX9 and FOXG1 in GBM pathogenesis, raises the possibility of future targeting strategies. Although drugs targeting these transcription factors have not yet been developed, this is an area of major drug development activity.
ecDNA Discovery
Thus far, all of the resistance mechanisms discovered in the various Cores, and discussed in this series, relate to how mutations or alterations to a specific gene or protein can create resistance in glioblastoma, as well as the potential roles the tumor microenvironment and metabolism can play. But the Biomarkers team found another astonishing mechanism of drug resistance that may also play an important role in why glioblastomas don’t respond well to most attempts to treat them.
Changes to key genes are well-known to play a role in the development of cancer, and because genes are typically found on chromosomes, this is often where cancer researchers assumed any cancer-causing genes (or oncogenes) resided.
But researchers from the Biomarkers team recently discovered that short, circular fragments of DNA containing oncogenes, that are separate from the DNA found in chromosomes, are present in a wider variety of cancers than previously thought, including approximately 90% of brain tumors. These small DNA particles are called, “extrachromosomal circular DNA” or ecDNA, and are almost never found in healthy, normal cells. Moreover, the researchers found that oncogenes (again cancer-fueling genes) are significantly more likely to be found on ecDNA than on chromosomes. In other words, ecDNA may play a far bigger role in the growth, diversity and drug resistance of cancer cells than genes housed on chromosomes in such tumors.
The team also demonstrated that tumors are more diverse (or heterogeneous) when oncogenes are active on ecDNA than on chromosomes, accelerating evolution in tumors that makes them more complex and harder to treat. This is because, unlike normally when DNA in chromosomes is passed down to “daughter cells” equally when cells replicate and divide (as they are constantly doing in the human body) through an orderly directional process, the circular less complex nature of ecDNA allows for genes to be amplified quickly and passed down in a more random manner. This enables tumors to more rapidly acquire and pass-on high levels of cancer-promoting oncogenes, and to do so in a way that greatly enhances cell to cell variability, enabling tumors to rapidly evolve. Tumors with lots of variability – called intra-tumor heterogeneity, meaning that even within the same tumor from the same patient, tumor cells might be subtly or even dramatically different – are more difficult to treat because if you target one type of mutation with a medicine, but it is only present in some of the tumor cells, then the remaining tumor cells without that mutation can still continue to grow.
Understanding how tumor cells evolve and how they increase the copy number and variability of their drivers is likely to yield some pretty important clues about the fundamental biology of cancer and how we might be able to target it.
Attribution: Dr. Mischel
Critically, the team now working to unearth the molecular mechanisms involved in the genesis and maintenance of ecDNA and exploring how ecDNA levels change in response to changes in the tumor’s internal environment. This could help uncover how ecDNA formation can be stopped before it drives tumor evolution and diversity, making cancers like glioblastoma extremely difficult to treat.
In addition to the results detailed above, the Biomarkers team:
Made a discovery that the nutrients glucose and acetate can activate a protein that re-programs a cancer cell’s metabolism, which causes tumors to grow rapidly and avoid targeted treatments. > Learn more
Working with the Drug Development team, is exploring the possibility of a clinical trial that combines a drug known as “ATO” with drugs that inhibit the EGFR pathway including a target known as mTOR which has been implicated in helping aid glioblastoma growth.
Discovered a mechanism whereby altered growth factor receptor signaling in GBM couples changes in metabolism with the ability to protect the tumor cells from damage against harmful metabolites. This enables tumor cells to adapt and survive changing nutrient supply levels and different environmental conditions. > Learn more
Summary and Moving Forward
During the course of their Defeat GBM work, the Biomarkers teams has published eight high profile papers in top science/medical journals. Each of these papers is already having considerable scientific impact. More importantly, a number of their findings are poised to make clinical impact for patients. They have identified new targetable mechanisms in glioblastoma, coupled with compounds that are ripe for clinical development and testing.
Moving forward, the team wants to continue the hunt for metabolic and epigenetic co-dependencies that could be used to find vulnerabilities within glioblastomas that could be targeted by drugs; continue to pursue the therapeutic strategy of breaking glioblastoma’s ability to uptake vast amounts of cholesterol to fuel its growth; and better understand and develop ways to possibly target ecDNA to treat glioblastoma patients.
*Note: Defeat GBM was designed with four cores. The three discussed in this series are the currently “operational” Cores, the ones that are doing “preclinical” research. The fourth Core – the “Innovative Clinical Trials” Core – is poised to take advantage of the studies the other Cores are performing, and the discoveries they are making, to develop clinical trials that are faster, more focused, and deliver the right medicines to the right patients at the right time (precision medicine!)